Mark Reed, DPM
DABFAS FAPWCA

714-528-3668










Neuropathy Cause & Treatment

Dr. Mark Reed began using nitroglycerin patches in 1989 as a Resident at UCSF / VASMSF to first treat diabetic ulcers to stimulate small vascular arteriole blood flow that resulted in increased ulcer healing rates. In using nitroglycerin to treat Wound Care patients, these patients with peripheral and autonomic neuropathy began reporting their peripheral and autonomic neuropathy symptoms were being reversed. Over the last 30 years, Dr. Reed has developed a nitroglycerin patch protocol that has reversed more than 3000 patients with peripheral and autonomic neuropathy and prevented countless diabetic ulcers from occurring.
For Diabetic Wound Care Information,
click here.
For Diabetic Foot Care Information, click here.
For Diabetic Nutritional Guideline Information, click here.
For Diabetic Foot Infection Information, click here.
For Diabetic Charcot Foot Deformity Information, click here.
For Peripheral Arterial Disease Information, click here.
DIABETIC NEUROPATHY (DNP) CHALLENGES AND NITROGLYCERIN
One of the most significant pathophysiology complications of Diabetes is neuropathy pain and or numbness that to date continues to represent a therapeutic challenge. Schreiber AK, et. al., Diabetic neuropathic pain: Physiopathology and treatment. World J Diabetes. 2015 Apr 15;6(3):714-528-3668. Doi: 714-528-3668/6. i3.432. Nitroglycerin has been prescribed for over 75 years to reverse oxygen ischemia causing angina pectoris by vasodilation of the microcirculation involving the arterioles. Nitroglycerin has been used for more than 33 years by Dr. Mark Reed to increase the microcirculation of the arterioles in the lower extremity in using nitroglycerin patches for 12 hours during the day that has the same effect on reversing the same angina symptoms in the feet in reducing or eliminating radiating burning pain in the feet. These findings were reported with significant reduction in pain in using transdermal nitroglycerin. Taheri A, Farbood et.al., “The effect of transdermal nitroglycerin on pain control in diabetic patients with peripheral neuropathy.” J Diabetes Metab Disord. 2015 Dec 1; 14:86. For wound healing, Dr. Reed has the patient place an additional patch proximal to the ulcer that increases oxygenation and white blood cell migration into the healing wound tissues.
NEUROPATHY DEFINED and TYPES
Diabetic neuropathy is a debilitating disorder that occurs in nearly 50 percent of patients with diabetes. Diabetic neuropathy in type 1 diabetes can present as a late finding after having the disease for more than five years and can be an early finding in type 2 diabetes. Diabetic and non-diabetic neuropathy are peripheral sensorimotor and autonomic. Sensorimotor peripheral neuropathy involves sensory symptoms of pain, paresthesia, numbness, paralysis, cramping, nighttime loss of balance and antalgic unstable gait. Autonomic neuropathy involves dysfunction of cardiac, genitourinary, sudomotor, endocrine and cerebral systems.
Patients may present with only one type of diabetic neuropathy or may develop combinations of neuropathies as distal symmetric polyneuropathy. Distal symmetric polyneuropathy is the most common form of diabetic neuropathy where a patient presents with numbness, tingling, and/or pain that begins in the toes and slowly spreads into the foot and up the leg. Because the symptoms are often present in the areas covered by gloves or stockings, peripheral neuropathy is often described as having a "glove and stocking" distribution of symptoms.
Autonomic neuropathy causes dysfunction of major organ systems responsible for sustaining life that we do not actively control. Autonomic cardiovascular neuropathy can involve silent cardiac ischemia, orthostatic hypotension, vasomotor instability, exercise intolerance, fatigue, heart rate arrhythmia, syncope, dizziness, lightheadedness, and balance problems. Autonomic Gastrointestinal neuropathy symptoms can involve dysphagia, gastroparesis, bladder dysfunction, bloating, nausea and vomiting, diarrhea, constipation, loss of bowel control. Autonomic Sudomotor (sweat glands) neuropathy symptoms can involve hyperhidrosis or excessive sweating, pruritus, dry skin, limb hair loss, calluses, and reddened areas. Autonomic Endocrine neuropathy symptoms can involve hypoglycemic unawareness. Autonomic Cerebral autonomic symptoms can involve sexual dysfunction, difficulty driving at night, depression, anxiety, sleep disorders, loss of food taste, decreased speech frequency and cognitive memory loss.
DIABETIC PERIPHERAL & AUTONOMIC NEUROPATHY CAUSES
Diabetic neuropathy is specific to the neuropathy caused from loss of oxygen to tissues and organs due to small vessel arterioles caused by excessive blood glucose. Diabetic neuropathy can affect any part of the nervous system and not just the skin of the feet as commonly believed. Diabetic neuropathy should be suspected in all patients with type 2 diabetes and in patients who have had type 1 diabetes for more than five years. In some instances, patients with diabetic neuropathy have few complaints, but their physical examination reveals mild to severe sensory loss to their forefoot and balance instability. Idiopathic (unknown) neuropathy has been found to precede the onset of type 2 diabetes or to occur as an early finding in diabetes.
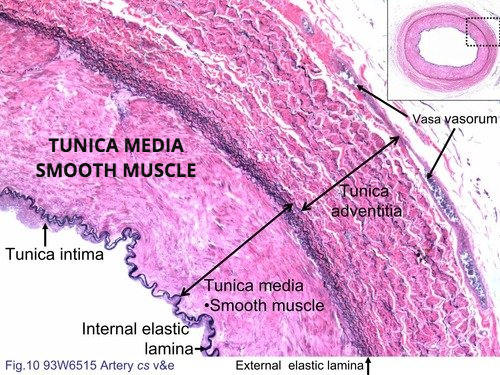
From an arterial standpoint, Diabetic peripheral neuropathy results from the somatosensory nerves in the skin becoming damaged from chronic high blood sugar that affects the small arteriole tunica medica smooth muscle. The arteriole tunica medica smooth muscles normally contract and relax in response to temperature and are the only muscle that can absorb glucose without insulin. When high blood glucose is occurring, the tunica medica smooth muscle absorbs glucose and then water follows to swell the wall of the arterioles and narrow the blood flow to the capillary that releases oxygen to the tissue.
Diabetes also causes Leukocyte dysmotility where the white blood cells swell and cannot move out of the artery to migrate to the location of an infection. In addition, dysmotility (not being able to migrate out of the arterial wall) occurs to fibroblasts (scar forming white cells) and osteoblasts (bone forming white cells). Thus, Diabetic patients who have uncontrolled blood glucose that results in osmotic swelling develop peripheral and autonomic neuropathy but also are immunocompromised to fight an infection as well as take a lot longer to heal soft-tissue and bone injuries.
When peripheral neuropathy becomes dangerous is when the nerves to the foot stop functioning and pain cannot be felt. This is known medically as the loss of The Protective Threshold of Pain. Clinically this is when a patient can no longer feel a Semmes-Weinstein monofilament (SWM) probe to their forefoot. The danger in losing the protective threshold of pain is the patient will get ulcers due to placing significant additional pressure on the forefoot to ambulate causing further loss of oxygen to the tissues.
Peripheral neuropathy will develop in about 60% to 70% of all people with diabetes as a national average. However, diabetic patients who control their blood glucose levels can reverse their type 2 diabetes and go into Diabetic Remission. Diabetic Remission is where the patient has achieved a Hemoglobin AIC level below 6 that usually is a combination of strict medication compliance and weight loss using intermittent fasting and or small portion dieting. If a Diabetic patient maintains their Hemoglobin AIC below 6, from a medical standpoint, they will stop a multitude of physiological processes that damage their tissues. Unfortunately, many patients intentionally skyrocket their glucose in eating known high glucose deserts and other foods like pastas and then inject additional insulin thinking there is no harm. Such hope is not lived long due to the irreversible medical consequences of giving yourself additionally insulin shots after skyrocketing your glucose that results in non-healing ulcers, dialysis, blindness and usually lower extremity amputations.
Non-DAIBETIC PERIPHERAL & AUTONOMIC NEUROPATHY CAUSES
Peripheral and Autonomic Neuropathy can be caused by many other diseases and conditions as follows: Alcoholism, kidney failure, vitamin deficiency (particularly B12 and folate), shingles (post herpetic neuralgia), Fibromyalgia, Complex Regional Pain Syndrome, Autoimmune diseases (Lupus, Rheumatoid arthritis or Guillain-Barre syndrome), AIDS, syphilis, and inherited disorders (amyloid polyneuropathy or Charcot-Marie-Tooth disease. In addition, neuropathy can be caused from exposure to toxins (heavy metals, gold compounds, lead, arsenic, mercury, and organophosphate pesticides), cancer therapy drugs (Vincristine, Oncovin and Vincasar), and antibiotics (metronidazole, Flagyl and Isoniazid). Rare causes of neuropathies include neurofibromatosis, congenital neuropathies (Fabry disease, Tangier disease, hereditary sensory autonomic neuropathy, and hereditary amyloidosis) and anti-cholesterol statin medications. In the extremities, peripheral nerve entrapments can cause peripheral neuropathy due to excessive pressure including tarsal tunnel syndrome in the ankle and carpal tunnel syndrome in the hand. Besides these many causes, many patients have no known cause and are diagnosed with idiopathic peripheral neuropathy.
WHAT ARE THE SYMPTOMS OF PERIPHERAL NEUROPATHY
Peripheral neuropathy is a disorder of nerve(s) apart from the brain and spinal cord. Patients with peripheral neuropathy may have tingling, numbness, unusual sensations, weakness, or burning pain in the affected area. Oftentimes, the symptoms are symmetrical and involve both hands and feet.
Autonomic Neuropathy can present with many differing symptoms depending on the nerve involved, including numbness, pain of different types, weakness, or loss of balance. Because the autonomic nerves control bodily functions that we do not consciously think of, such as heart rate, digestion, and emptying of the bowel and bladder, autonomic neuropathy manifests with symptoms affecting the loss of control of these functions. Symptoms may include problems with blood pressure, voiding, passage of stools (diarrhea, or constipation), heart rate, or sweating. Cranial neuropathy is similar to peripheral neuropathy, except that the cranial nerves are involved. Any of the cranial nerves can be involved. One of the more common causes of cranial neuropathy called ischemic optic neuropathy is loss of blood flow from the optic artery to the optic nerve.
Specific nerves can be involved in neuropathy. When a specific nerve is involved, the symptoms are limited to the distribution of that nerve. The most commonly involved peripheral nerve is the posterior tibial nerve in the ankle called tarsal tunnel syndrome or the median nerve at the wrist called carpal tunnel syndrome. Essentially any peripheral nerve can become entrapped and cause the signs and symptoms of neuropathy. Surgical excision of nerve tumors or neuromas can result in neuropathy when the cut nerve cannot reconnect and an amputation neuroma resulted that present with constant, burning, radiating, tingling type pain. Trauma can also affect nerves that are susceptible to traumatic injury such as the ulnar nerve is commonly entrapped at the elbow, the peroneal nerve to the outer part of the knee, the pudendal nerve in the pelvis and lateral femoral cutaneous nerve at the waist.
WHAT TESTS DIAGNOSE PERIPHERAL NEUROPATHY?
Because peripheral neuropathy has so many causes and so many presentations, the first step to diagnosis is performing a thorough medical history and physical examination. Certain tests done during the physical exam, including vibration and Semmes-Weinstein monofilament testing, are very accurate in diagnosing certain types of peripheral neuropathy, such as peripheral neuropathy seen with diabetes. In addition, 50% of Diabetic type 2 diabetes who have neuropathy have associated large vessel peripheral vascular disease that involves narrowing or stenosis of the large leg arteries. If you have type-2 diabetes and have neuropathy, it is important to ask your doctor to evaluate your large vessels in testing your lower extremity pulses and to have the doctor order a doppler vascular lower extremity study if warranted. Early diagnosis of large vessel peripheral vascular disease and corrective vascular intervention is important to treat this limb and life-threatening medical condition before a foot ulcer and resultant infection occurs.
The Capillary Refill Time (CRT) tests the refill of blood to the skin to pressure proving there is a small vessel vascular pathology. Sensory testing of patients with diabetes is an integral part of preventing new and recurrent foot ulcers. The Semmes-Weinstein monofilament (SWM) test is used to screen for loss of protective sensation and if a positive test is noted in an examination, peripheral arterial doppler testing should be ordered to rule out peripheral vascular disease. Blood tests for exposure to toxins and electrodiagnostic studies, such as nerve conduction studies (NCS) and electromyography (EMG) are also useful. Either skin biopsies or quantitative sudomotor axon reflex testing (QSART) is used to help diagnose different types of neuropathies.
TREATING AND REVERSING PERIPHERAL NEUROPATHY!
The treatment for peripheral neuropathy first must be focused if a treatable cause can be diagnosed in assessing the medical history, clinical findings and then perform appropriate laboratory tests due to the many causes of neuropathy as discussed above. As a fundamental treatment, a patient with neuropathy should have an evaluation by their Primary Doctor to ensure their diabetes is controlled and any other major medical issues are addressed. Dr. Reed also recommends diabetic patients adopt an intermittent fasting program every day that skips breakfast to decrease the dependency on glucose and insulin and to burn fat to maintain the metabolism. Controlling diabetes will prevent the progression of neuropathy. Where local causes of neuropathy are diagnosed these are corrected such as peripheral nerve entrapments including tarsal tunnel syndrome or carpel tunnel syndrome using physical therapy, alcohol injections, and or surgery. Where systemic causes are diagnosed, these issues are also addressed.
For Diabetic and non-Diabetic peripheral and autonomic neuropathy, Dr. Mark Reed has been using nitroglycerin for 30+ years to treat peripheral and autonomic neuropathy. Nitroglycerin has a mechanism of action of vasodilatation of the Tunica Media smooth muscle of the small arterioles that increases blood flow to the capillaries responsible for oxygen release to the surrounding tissues. This arteriole vasodilatation due to the nitroglycerin reverses the oxygen tissue damage from narrowing of the arteriole lumen due to excessive glucose osmotic swelling or from unknown causes in idiopathic neuropathy.
Dr. Reed assesses the effectiveness of nitroglycerin using the Capillary Refill Time as well as the temperature of the forefoot that is abnormal in diabetic and idiopathic neuropathy. Each patient has a different sensitivity to nitroglycerin. However, for most patients who are stared on a loading dose of nitroglycerin, their ischemic pain and related paresthesia disappear within the first week of administration. As the loading dose is adjusted for each patient, a therapeutic dose based is reached based on their Capillary Refill Time (CRT) becoming normalized. Once a therapeutic dose is reached, almost all patients experience over the next three to five months skin nerve regeneration as feeling increases in the feet and their confidence in walking improves. This response is most significant in patients with normal physiology with no underlying health issues who have peripheral neuropathy from fibromyalgia or cancer chemotherapy treatments. Besides nitroglycerin causes the increase release of oxygen from the capillaries to the nerves of the skin, there is also reversal of autonomic neuropathy symptoms in providing increased capillary oxygenation to major organ systems such as the eyes, kidney and brain. Based on Dr. Reed prescribing nitroglycerin for Diabetic patients for 30+ years and observing their long-term medical benefits, Dr. Reed placed all neuropathy patients on lifetime regiments. Such a lifetime regiment combined with controlling diabetic blood glucose levels will help prevent peripheral and autonomic neuropathy to varying degrees and helps prevent foot ulcerations.
There are many medications that help a patient manage the pain or discomfort of having painful or numb feet and or autonomic neuropathy complications. However, none of these following medications actually cure the underlying small vessel oxygen damage from excessive blood glucose from diabetes. Topical application of Capsaicin, (the chemical in chili peppers gives a hot feeling) and menthol liquids and creams are available over the counter to help distract the feeling of the pain of peripheral neuropathy.
PREVENTATIVE INTERVENTION
When a patient cannot feel pressure or pain to their feet, this is known as the Loss of the Protective Threshold of Pain, that requires the patient to adopt numerous preventative interventions. These would include looking at their feet every day, restricting walking to 30 minutes with 5 minutes of rest to revitalize the skin to the bottom of the foot, protective diabetic shoes with pressure reducing insoles, never walking barefoot around the house, three-month checkups with the Doctor managing your diabetes and bimonthly visits to the Foot Specialist. In addition, if a prominent callous or purple callous is observed, the patient must not wait but make an urgent appointment with a Foot Specialist and limit weight bearing as much as possible.
EXERCISE CAN REDUCE NEUROPATHY PAIN
Low impact exercise can reduce the pain from peripheral neuropathy due to increased tissue oxygenation. If you have not exercised in some time, plan to a gradually ease into an exercise program over days and weeks. As you slowly improve you should set a goal to exercise about 30 minutes a day alternating days to allow your body to recover.
Before staring an exercise program, you should discuss your plans with your Doctor to insure there is not issues based on checking the status of your heart, eyes, kidney and feet. You should also discuss with your doctor what glucose levels you should have in testing your blood glucose before and after exercise and what you should do on a sliding scale if glucose levels go too high. In addition, it is important to have a source of glucose available during exercise such as hard candy if your glucose drops to low.
Low–impact exercises that do not place excessive pressure on the bottom of the feet are usually well-tolerated by diabetic patients. Exercises such as swimming, water aerobics, recumbent bicycle riding, rowing machine, and yoga are usually good choices. High-impact exercises may actually make peripheral neuropathy worse or cause further nerve damage due to the excessive pressure placed on the feet to balance with neuropathy.
BALANCE EXERCISES
Balance is a learned neuromuscular skill that improves with practice. Balance exercises should be performed at least once-a-day every day. On average, after six weeks of balancing every day, patients will report a marked improvement in balance control and confidence in their ability to walk. Before balancing, place yourself in front of a counter to so both hands can grab the counter if you begin to lose your balance. Balance on one foot at a time for 30 seconds and alternate for ten times. As balance improves, the duration should be increased to one minute on each foot for five times. If you cannot actually balance on one foot, then lift the heel of one foot while balancing on the other for 30 seconds.
In addition to balancing each day, standing on your tip toes should be also performed. While standing in front and holding onto a countertop, raise up on both toes and hold the position for 30 seconds. Repeat standing on the toes for five times with the goal to increase standing on your tip toes for one-minute for five times.
NEUROPATHY SCAMS
There are many scams ongoing by so called Neuropathy Experts. These Neuropathy Experts have no training or scope of practice to treat diabetic patients or any patient with neuropathy. Neuropathy treatment is covered by Medicare so there should never be a payment made for a special non-covered treatment. Typical neuropathy scams involve free dinners with high-pressure sales fear tactics with fake paid testimonials trying to con $8,000 to $12,000 from mostly elderly victims. Treatments involve heat lamps, lasers or vibrators or amazing vitamins and herbs with fake medical research.
DISCLAIMER: MATERIAL ON THIS SITE IS BEING PROVIDED FOR EDUCATIONAL AND INFORMATION PURPOSES AND IS NOT MEANT TO REPLACE THE DIAGNOSIS OR CARE PROVIDED BY YOUR OWN MEDICAL PROFESSIONAL. This information should not be used for diagnosing or treating a health problem or disease or prescribing any medication. Visit a health care professional to proceed with any treatment for a health problem.

Mark Reed, DPM
DAPFAS FAPWCA
1275 N. Rose Drive, Suite 136
Placentia, CA 92870
Open M-F 8:30 to 5
Saturday: By Appointment
Info@Podiatry.Care
Fax: 714-528-0739
Office: 714-528-3668
Located in the
Placentia Linda Hospital
Medical Building
Follow Dr. Mark Reed

*****
Beckie Burcham.
An absolutely amazing and genuine doctor who is not interested in only treating the symptoms, but rather treating the real cause! Dr. Reed explains everything in real simple terms that anyone can understand, especially seniors. He has amazing, common sense solutions (i.e. treatments) for unresolved diabetic foot ulcers where others have only wanted to continue cutting weekly into my family member's foot! Dr. Reed is absolutely AMAZING! And if you are getting no where with your currents foot issues or someone continues to only cut, please, please...do yourself a favor and contact Dr. Reed's office right away! Trust me, my family member has been dealing with an unresolved diabetic foot ulcer since 2018, and in just 3 weeks the foot is healing fantastic!!! Thank you Dr. Mark Reed. You have helped us to save the foot!!!
What an Amazing Podiatrist Dr. Mark Reed is! After years of other foot doctors just cutting into my family member's foot (diabetic foot ulcer), with numerous infections along the way...I did research and found Dr. Reed. Absolutely the best decision I have made for my loved one! After only 3 weeks of treatment, the foot ulcer is healing!!! No amputation! No continuous cutting and keeping the wound open and susceptible to infections! Brilliant man with great knowledge, kind heart, straight to the point and tells the truth the way it is! Dr. Reed does not just treat the symptoms, but rather the source of the problem! My family member's glucose levels are down to an average of 112 now. The wound is healing and new skin is growing!!! Amazing! I would highly recommend Dr. Reed to anyone and everyone! Thank you Dr. Reed, from the bottom of my heart! You have been a God send! Thank you!
*****
Mathew
H. I went to Dr. Reed because I had a chronic (5 months) wound on my leg that needed expert medical attention. Dr. Reed assessed the wound and knew how to treat it. He explained the process of healing the wound and what I needed to do in order to make the plan work.
I appreciated that Dr. Reed took the time to explain the process and his approach to me. As I followed the plan, I saw improvement within the first week and continued improvement in the following weeks. Within six weeks of my first appointment, the wound was healed.
Dr. Reed is personable and I enjoyed speaking with him in conversation. Most importantly, he told me what the treatment plan was, why it was that, and what I needed to do to ensure that it is effective. I am reluctant to go to doctors. I highly recommend Dr. Reed because he understands that many people feel that way and most importantly because the treatment was successful.
Lastly, the office staff are professional and kind. Dr. Reed's office is a first class group and I recommend them very highly.
*****
Paul Gordy. Dr. Reed is an outstanding podiatrist...he is state of the art medicine. This is by far the most kind, compassionate and caring physician who takes personal interest in his patients care and success in healing...when Care More and BlueShield doctors said they could not heal me...Dr. Read said "that's crazy", I'll heal you in 90 days .....and he DID!!!!!,
Amazing skill. You will not find a better person or doctor anywhere...
My family and I. Love Dr Reed.
You will too!
Paul Gordy
Yorba Linda Ca
*****
David M. The entire staff is friendly and very helpful. Dr. Reed is dedicated, spends time to take care of his patients. I had gangrene in my toe and Dr. Reed was diligent in his care and was able to eradicate the problem. I have recommended him to others, who had similar positive experiences.
***** Lee Godden. I have nasty bunions which eventually led to a painful stress fracture of the second metatarsal while playing basketball 2x/week. Dr. Reed managed my entire recovery, from initial visit to discharge two months later. He took X-rays and did ultrasound therapy. I was happy that his focus was on realignment and patient education, as opposed to surgery. I'm now running again thanks to the orthotic insoles, toe spacers, etc. that Dr. Reed put me in. I highly recommend Dr. Mark Reed.
***** Yvon Cariou. Dr. Reed did a great job on that ingrown toe nail, a painful condition. It took some time but Dr. was persistent and supported the process with detailed explanations and supplemental care as needed. A good office to go to.
***** Sue Alexander. If you’re looking for a podiatrist (foot and ankle doctor), may I suggest Dr. Mark Reed in Yorba Linda. Throughout my treatment Dr. Reed explained what he would be doing and why. Thank you Dr Reed for your expertise, kindness and encouragement! Sincerely, Sue Alexander
***** Salam Hamad. Hat off for Dr. Reed. He was the 4th doctor, second specialist to consult for my Plantar Fasciitis case. I went to him after the 1st specialist, using injections, boots and what not decided to operate on my heel in 30 days if the pain does not go away. Doctor Reed threw all that talk away and dismissed every recommendation. I went to him armed with lot of documents, dates and details of what the first 3 doctors did. He said, don't give the history, just tell me where it hurts. He examined the heel and the foot and diagnosed the problem immediately. He then prescribed the method to treat it. He did it! yes, it took more time than he thought but he DID it. I owe doctor Reed and appreciate him, his knowledge, experience and his caring attitude every time I walk. Yes, walking became possible for what he did. Oh! by the way, he is not in it for the money.
***** Sue Alexander. If you’re looking for a podiatrist (foot and ankle doctor), may I suggest Dr. Mark Reed in Yorba Linda. Throughout my treatment Dr. Reed explained what he would be doing and why. Thank you Dr. Reed for your expertise, kindness and encouragement! Sincerely, Sue Alexander
***** Monsie Crane.
Dr Reed cured me of the neuropathy in my toes. The neuropathy was a result of chemotherapy, which I received as a cancer treatment. He also helped me with proper shoe fitting for bunions and longer second toes. I highly recommend Dr Reed.
***** Colleen Livermore. Dr Mark Reed has been an excellent doctor, evaluating my foot and ankle pain, and giving me the instruction and exercises needed to strengthen and heal. I appreciate his excellence, expertise and experience. Ankle pain can be so challenging so to feel better after his help is a great relief.
Reply1
*****
Matthew Jones.
Dr. Reed has been my podiatrist for approximately 2 years now. He remains one of my favorite doctors because of how kind he is, how punctual he is and most importantly how effective he is.
I have been to several other podiatrists in the past and I just about gave up until I found Dr. Reed on google. The results he has given me have changed the way I feel and the way I look.
***** Lily Lambutu. Dr. Reed is an excellent doctor. He listens, gets straight to the point, explains everything, and pays attention to detail. He answers all questions honestly. I've seen him for ingrown toenails and a tumor on the bottom of my foot. I trust him completely as he takes the time to assess the issue and will take a conservative approach if it will solve the problem.
***** Bryant Brislin. Dr. Reed took a thoughtful approach to my issue and came up with a solution that other podiatrists had not. He took his time and was very friendly, which was refreshing. He seemed to truly care for me to get better!
***** Lisa Fogerty.
Dr Reed is an outstanding doc. Several years ago I had a hammer toe surgery done by another doctor who damaged the nerves in my foot. I was in pain for 3 years and was told by that doctor that I would have to live with it and that eventually the nerves would heal. They didn't. I couldn't sleep due to the pain and had to alter my exercise routine. Dr Reed took on the case, correctly diagnosed the problem and started a program of injections to get the nerves to regenerate. He told me to be patient and that "we" would fix the problem. He always kept me informed of the procedures and made me part of treatment plan. It took several months but today my foot and toes are healed thanks to Dr Reed's persistence.
My wife dislocated several toes in an accident and was in significant pain. Dr Reed fixed her up as well.
We are both very grateful to Dr Reed and his excellent staff for their kind and professional medical services and highly recommend him. If you want the best podiatrist in Orange County you found him in Dr Mark Reed.
***** Samantha Smith. It’s been almost 2 years since Dr. Reed cut off an amputation stump neuroma and then reconnected my husbands medial plantar nerve. This man has changed our lives forever. After being turned down and rejected by SO many doctors, we had no hope left...then we found Dr. Reed. He really did the impossible! My husband was in so much pain for so long and now feels little to no pain thanks to our friend Dr. Reed. We owe everything to him and will always be SO thankful for everything he has done for us. He will forever be a huge part of our lives.
Reply1
***** Leo Burke. I'm an avid hiker but have been plagued for years by a large toenail that was sensitive to pressure and would have to go to great lengths to avoid losing the nail. But every now and then I would lose the nail and all this was impacting my hiking (and ruining some vacations). I was seeing other podiatrists and we would try various work-arounds, but I finally decided that I would get rid of that nail once and for all. I had a lot of trepidation about that, but I decided to see Dr. Reed to consult with him on doing so. He assured me that it would be no problem at all, which surprised me, so I agreed to have him do the removal. Amazingly, it turned out to be a piece of cake with little to no pain, and I was back in action very quickly. It pains me to realize that if I had seen him a long time ago I could have avoided years of aggravation and frustration. Not only that, but he's an expert on hiking boots and given me a lot of help in boot selection.
He's been in this for so long that he's a fountain of knowledge and enjoys imparting his wisdom to his patients. For example, I also have a pressure sensitive small toe on my other foot and he was able to give me samples of some products that can relieve pressure on the toe that I hadn't been aware of. If that doesn't do it, I can cut an "X" in the boot over that area and cover it with a piece of leather. He then supplied me with a piece of leather that could be used for that purpose and told me what glue to use.
There's no question about it - Dr. Reed is the man to see for your foot problems. He's head and shoulders above everyone else.
***** Gloria Gonzalez. Dr. Reed is a great podiatrist. He's the only doctor that has helped my family's and my foot issues. He didn't suggest surgery for my issue, and his solution was easy and innovative. A couple of years later, and his solution still works.
Reply1
***** Nikki Clark. I have been a patient of Dr. Reed's for 6 months. During this time I have found both his professional staff and Dr. Reed to apply the utmost patience, compassion and expertise. They always make time for appointments and during doctor visits. Dr. Reed has an impeccable bedside manner, provides all options available and genuinely cares for a positive solution. Dr. Reed is a student of his practice and applies current medical advancements. I would recommend Dr. Reed and his staff to family and friends for problems they might be experiencing.
*****
Viet Tieu Bao: I have a great experience with Dr. Reed. First of all, he's an awesome surgeon as it turned out i didn't have any pain after my surgery (i had a tumor that grew next to my Achilles tendon that needed to be removed and in order to have a clean removal of the tumor so it won't come back Dr. Reed had to shave off 1/3 of my Achilles tendon). Amazingly i did not have to take a single pain killer. Hats off to his skills. Secondly, his caring is extremely important since he encouraged me to call him anytime if i have a concern or just a question. I did call him on the day of the surgery i noted the time 11:30pm and he did return my call just few minutes later. I was amazed how pleasant and calm he was even though that late in the night and he ensured me that i feel ok before he let me go back to sleep. Last but not least, he is very detail oriented surgeon as he always explained clearly his procedure & options & pros & cons as well as any medical terms that i don't understand. I feel i was so lucky that I chose Dr. Reed for my problem and i highly recommend anyone who needs a DPM should give it a try with Dr. Reed. Am confident that you won't be disappointed.
Thanks Dr. Reed for taking good care of me and deeply appreciated for all you did for me.
***** Uli H. Went to Dr. Reed about 2 months ago because I woke up with excruciating pain on top of my foot. There was no injury or even exercise the day before so it was totally random. I explained this to Dr. Reed and he diagnosed it as tendinitis. He explained to me why it happens and it made perfect sense. So in one session I basically found out that I've been wearing the wrong shoes for my flat feet this whole time. What a difference my life would've been if I had visited him years ago. He told me my knees are not aligned correctly because of my flat foot which explains my knee pain. He referred me to a place to get some better walking shoes and showed me creases on my shoes that showed just how much pressure is on one side of my foot. The custom orthotics he made me have been a life changer. The only way I can describe the feeling is I use to feel like I was walking on unstable stilts and now my feet have custom made platforms and I'm stepping on a solid foundation every step. The night splint he gave me was the solution to the tendinitis. It is now gone and even played soccer within a month of first going. I'm now working on my pre-existing ankle injury and have to test out my tendonitis ankle to make sure its completely gone. Dr. Reed is great, has some great advice and I definitely recommend him.
***** Douglas Ho. I am a returning customer after many years. Returned to Dr Reed to evaluate my Plantar Fasciitis. He recommended stabilizing tennis shoes and a night boot to keep my foot in position. He said I have a mild bursitis on my heel. His recommendations are spot on and I am slowly recovering. His background in Sports medicine was also helpful in commenting on a treatment for my tennis elbow. I love it.
***** Richard Baugh. Dr Reed has helped me excellently over the years to overcome several different foot problems: ingrown toenails (his treatment was painless!), neuroma and plantar fasciitis. He is friendly and takes the time to explain causes and treatments. I’m most grateful to him and will continue to use his services.
**** Victor Skillings. It was a phenomenal experience from the initial consultation, pre-surgery preparation, surgery and follow-up visits. Now, I know why so many of his patients feel compelled to write great reviews about Dr. Reed. His approach to patient care, willingness to explain the procedure and answer all your questions, surgical skills and genuine interest in his patients were far, far better than what I had expected.
I had bunion surgery about two months ago. It was extremely large, about the size of a walnut. My procedure took a little more than an hour, and to my amazement, I felt absolutely no pain during or anytime after the surgery. In a few weeks, I was able to walk fairly normally.
In summary my review is five out of five stars, thumbs up, A+, highly recommended and all the above! So if you’re looking for the best foot surgeon in Orange County, look no further – Dr. Mark Reed should be your first and only call.
***** Juan Vallejo. Okay I'm a very critical. This Dr and his office staff are hands down the best. I had a great experience with Dr. Reed. I have recommended him to all the people I know. Everyone is great and professional.
***** Karina Lerma. He is the BEST Podiatrist in Orange County. He truly cares for the patients and tries to give them the best treatment!
© 2015 PLFAG. All rights reserved.



***** Juan V in Canyon Country, CA. Okay I'm a very critical. This Dr and his office staff are hands down the best. I had a great experience with Dr. Reed. I have recommended him to all the people I know. Everyone is great and professional.
***** Laila in Yorba Linda, CA. After visiting 2 other doctors in a period of 2 years, with no success. Dr. Reed was able to pinpoint the problem with my feet! Finally, I have no pain while running and working out.
***** Pam L in Villa Park, CA. I am so pleased with the results of Dr. Reed's care of my daughter's foot pain while wearing her figure skates. She has figured skated for a few years, and recently developed arch pain while wearing her skates that would not go away no matter what she did. He made custom orthotics to fit in her skates and support her feet, and she is currently pain free! If you have an athlete or figure skater, I would definitely recommend Dr. Reed for podiatry care.
***** J. Barna in Blue Jay, CA. I've had an amazing experience with Dr. Reed and his office staff! I was in significant pain from a neuroma when I first came to his office. Dr. Reed was my second opinion, because the first office, turns out, had no idea what they were doing. Dr. Reed was able to reduce my pain until I needed surgery. After a short recovery I am now near 100%!! I would recommend Dr. Reed to anyone in Southern California that is suffering from any type of foot appointment.

***** Cher Corso. My fourteen year old daughter (a dancer) was having problems with both feet. We had already been to one podiatrist with no satisfactory resolution when we found Dr. Reed. The entire experience was positive for our entire family. Dr. Reed knew exactly what was going on and corrected the problem. I have already recommended Dr. Reed to a very dear friend who's son is having foot problems. This is the place to go! Great experience for my daughter who was scared of doctors before seeing Dr. Reed.
**** May Liping. I had a painful bump on the top of my foot for months. My previous podiatrist, misdiagnosed me and scared me half to death. First he claimed my ganglion cyst was caused by my wearing bad shoes. Then, when my foot continued to hurt and I saw him again, he claimed the cyst "had hardened" and therefore, only surgery could remove it. He made this declaration without even x-raying my foot. Scared, I went to Dr. Reed for a second opinion and thank God I did. Dr. Reed did an x-ray and determined that the cyst could be treated immediately. He looked stunned when I told him about the other doctor's diagnosis. He told me that, soft or hard, cysts can be taken care of. He gave me an injection of steroids and the cyst has disappeared ever since. Dr. Reed saved me from unnecessary surgery and for that, I will always be grateful!
***** Linda Rodgers. Dr. Mark Reed was the second doctor I went to for my ingrown toenail. The first foot doctor did not do the procedure right and the ingrown nail returned. The pain from the procedure was also terrible and I do not think the doctor understood what she was doing because she was saying that it is supposed to hurt. Dr. Reed took a lot of time to explain the procedure and reassure me that the injection was going to go smooth. Dr. Reed used a skin vibrator that made the shot painless and I did not feel anything as to the needle and the numbing of my toe. Dr. Reed talked about a number of interesting topics so the procedure was done and felt like it only took a few minutes. The office is very clean and the staff is great. There is not a better doctor out there for foot care. I highly recommend that you go to this doctor.